Yes. In fact the exact same condition that causes ‘runner’s knee’ is also be called ‘moviegoer’s knee’…well if that’s not confusing…
Both ‘Runners knee’ and ‘moviegoer’s knee’ refer to a condition called patello-femoral pain syndrome (PFPS), which is not in itself a very meaningful name. It really just means ‘mysterious knee-cap pain’ and is often a diagnosis of exclusion; one that is left once all others have been ruled out.
Why is it called runner’s knee?
The term ‘runners knee’ is used because the condition is most commonly found in runners. The problem with this name is that runners can suffer from other types of pain, like iliotibial band syndrome or arthritis, which aren’t technically PFPS. It can also be confusing because many non-runners also suffer from patella-femoral pain, such as cyclists, walkers, yogis and even officeworkers who sit all day (thus the alternative name, moviegoer’s knee’).
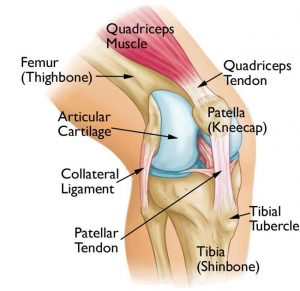
Image from – https://www.therapia.com.au/
So what is patellofemoral pain syndrome?
PFPS is knee pain that is felt mostly at the front of the knee – usually under or around the sides of the kneecap. Pain is often aggravated by stairs or hills and is often worse after sitting for long periods of time.
What causes it?
This is where things can get tricky. There is not often just one cause of PFPS in any individual; rather a number of contributing factors that are likely to differ from one person to the next. Some possible contributing factors can include:
- Muscle weakness (eg. quads or glutes)
- Poor control of movement (eg. control of knee bending or trunk control)
- Biomechanics (eg. kneecap position, excessive foot pronation)
- Reduced flexibility (eg. ITB, hip flexors, hamstrings)
- Overuse or training error (eg. too rapid a progression of mileage or hills)
So how is it treated?
The most important part of treatment is a comprehensive assessment. There is no recipe that can be followed because it will depend on what a person’s unique contributing factors are. For example, quads strengthening exercises might help for someone whose quad weakness is contributing to their knee pain, but might not help for someone whose main problem is hamstring and calf tightness, or weakness of their hip stabilisers.
Generally, to treat PFPS, we must:
- Settle the symptoms
- Stop the things that are aggravating (temporarily!) This might mean you stop running, kneeling, squatting for a few days until pain has settled.
- If pain is bad, you can try icing, anti-inflammatories, or heat if ice doesn’t work.
- Identify what is wrong
- this is where we come into it! You need a thorough assessment from someone experienced in managing knee pain. This will help identify the factors contributing to YOUR knee pain, which might be unique to you.
- Remedy the contributing factors
- this will likely include some exercises but may also include new shoes, temporary taping or technique correction
- Reload the knee and return to activity
- this will need to be gradually and carefully to avoid reaggravation.
How long will it take to get better?
This will depend on how early and well it is treated and how often it is aggravated. Some are better within a couple of weeks, whilst others can struggle with it for more than a year if left untreated. The key is to get it assessed early by someone who knows what they’re doing!
* GLOW Physio is highly experienced in the treatment of all types of knee injuries and can help you get back to whatever it is that makes you happy (running and moviegoing are both perfectly acceptable)! *
Recommended reading from Glow
5 habits for a happy, healthy spine!
Exercising with your Menstrual Cycle
Are high heels really that bad for you?